Salicylate-poisoned patients can be incredibly complex and severely ill. Secondary to the significant acid-base abnormalities that can accompany salicylate poisoning, hemodialysis (HD) is sometimes required to facilitate removal and correct acid-base status. In addition, if intubation is needed, hyperventilation on the vent is crucial to match the patient’s minute ventilation prior to insertion of the endotracheal tube.
A new study from the Illinois Poison Center evaluated the relationship between salicylate level, intubation, HD, and mortality.
What They Did
- Retrospective, observational study of poison center records.
- Intubated patients with a salicylate level > 50 mg/dL were included.
- Survival was compared to measured serum salicylate level and the administration of HD.
What They Found
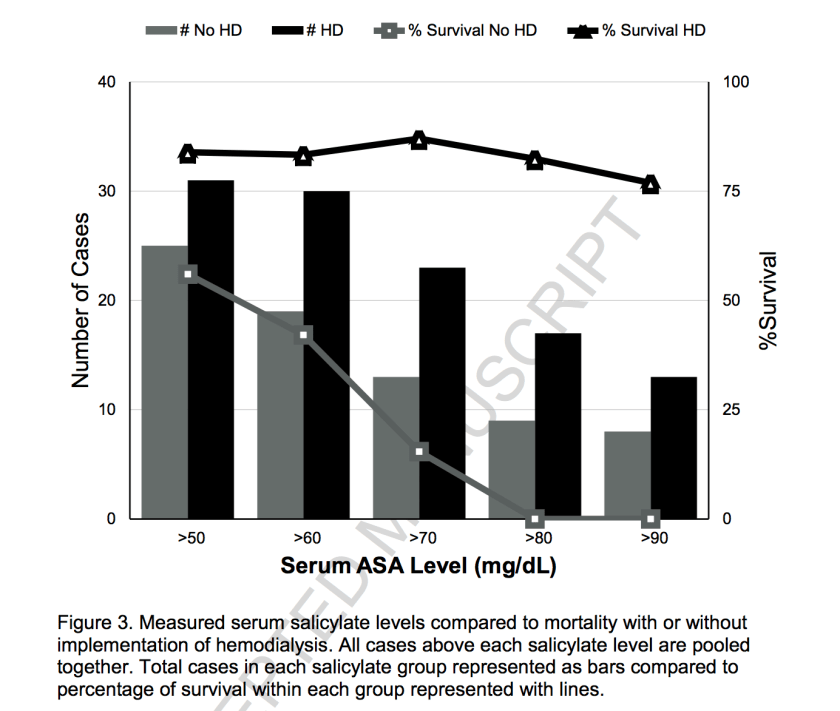
- Overall survival rate was 73% in the 56 cases reported
- In patients that did not receive HD:
- ASA level > 50 mg/dL had a 56% survival rate (14/25)
- ASA level > 80 mg/dL had a 0% survival rate (0/9)
- When patients received HD:
- ASA level > 50 mg/dL had an 83.9% survival rate (26/31)
- ASA level > 80 mg/dL had an 83.3% survival rate (15/18)
Application to Clinical Practice
- Even taking into account the retrospective nature and incomplete data sets from voluntary reporting to poison centers, there is an association between hemodialysis and survival in mechanically-ventilated, salicylate-poisoned patients with levels > 50 mg/dL.
- Early hemodialysis should be arranged in salicylate-poisoned patients who require intubation (or are headed in that direction).
- While it may seem like an obvious treatment strategy, it is clear from these records that patients are not receiving early HD when it may be indicated.
Reference
McCabe DJ, Lu JJ. The association of hemodialysis and survival in intubated salicylate-poisoned patients. Am J Emerg Med. 2017 Apr 10. Article in Press. DOI: http://dx.doi.org/10.1016/j.ajem.2017.04.017
